Health inequalities are particularly apparent in childhood asthma. OneNorwich Practices are looking to tackle this by re-thinking how we can make it easier for families to attend their annual reviews and therefore empower optimal self-management. Asthma clinics have been held in 10 schools in deprived areas of Norwich and the positive results have secured funding from the Integrated Care Board (ICB) to expand across Norfolk and Waveney. We have also been shortlisted for a national award for challenging health inequalities. Read on for our initial findings within the targeted Norwich schools and the rationale behind the project.
Background
Evidence suggests that:
- Emergency admissions for asthma in children and young people are strongly associated with deprivation, with significantly higher hospital admissions in poorer families.[1]
- However, children from deprived areas are less likely to attend preventative asthma reviews[2]
- If we can get hospital admission levels from the most deprived decile to match the least deprived, we could save the NHS 8.5 million, a year, in England alone[3]
The National Review of Asthma Deaths, (NRAD) in 2014, highlighted that two-thirds of asthma deaths are preventable, with annual review attendance being a key influence.[4] Self-management including provision of a personal asthma action plan (PAAP) and supported by regular medical reviews, almost halves the risk of hospitalisation, and improves markers of asthma control and quality of life.[5]
However, Asthma and Lung UK noted families reporting significant challenges accessing their surgeries for reviews.[6]
Levy, 2021, also notes, “Sadly, despite the NRAD report highlighting ongoing preventable factors for asthma deaths, the UK’s poor record of childhood asthma care persists with many examples of preventable asthma attacks and preventable childhood asthma deaths”.[7]
If we address these factors, we can reduce the risk of death.
Focus
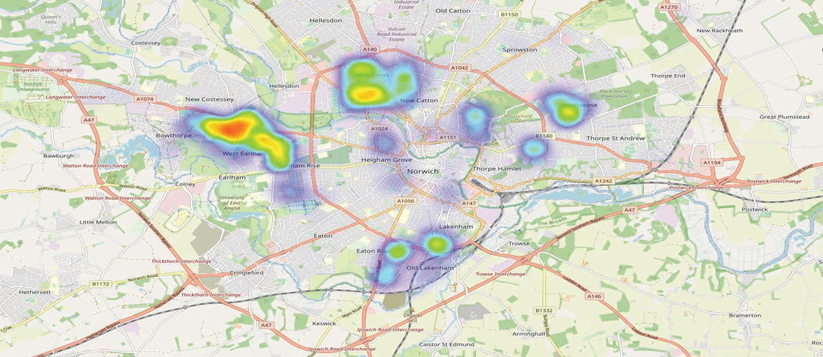
The heat map below indicates the high levels of childhood asthma associated with deprivation in Norwich[8].
The asthma clinics in schools project was developed based on these principles. We wanted to make it easier for families in deprived areas to attend their annual asthma reviews, and hence trialled holding them in schools. The feedback was phenomenal from both families and from schools.
Findings
Initial response
Families reported challenges with obtaining reviews at their surgery and welcomed the new approach: When the schools initially contacted parents some of the comments were:
- “Usually attends the GP but can’t remember the last time they went because of Covid restrictions”,
- “Very pleased as mum feels appointments at GP tricky”,
- “Great idea as difficult to get into GP surgery”.
Parents were keen to attend and even in the initial school, the uptake of families whose child was on the asthma register was excellent, achieving 81% engagement.
Family knowledge improvement
Self-reported confidence and knowledge in prevention and management of attacks grew significantly post school clinics: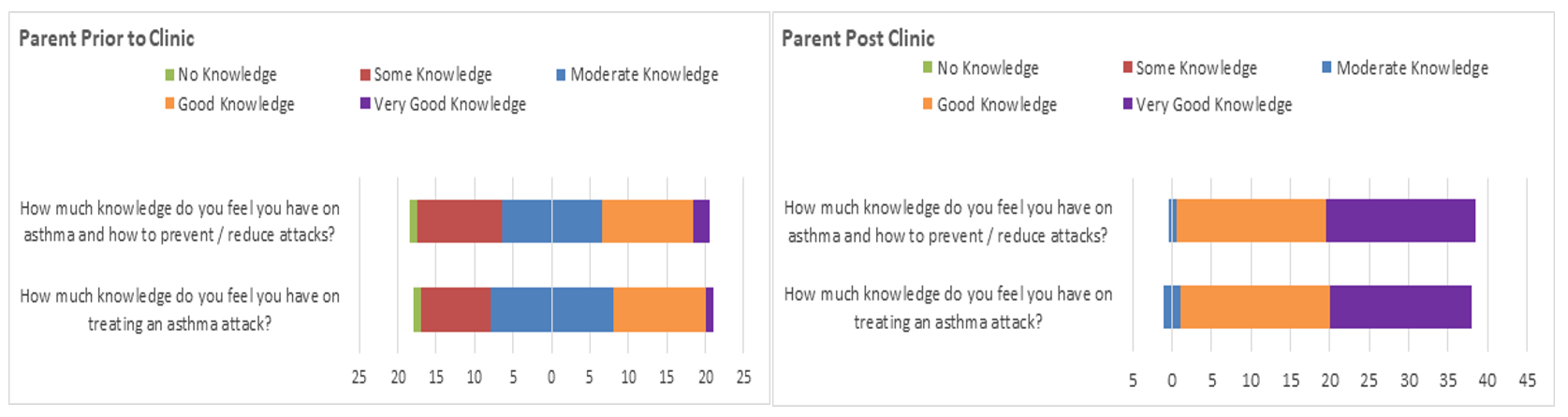
Unmet needs among school staff identified
Following a near miss, (“thank goodness you’re here”) it became apparent that school staff receive minimal training on asthma despite being responsible for 2-3 children per class with asthma. Therefore, asthma training became an additional key role, either face to face or through e-learning and currently each school now receives the Tier 1 Children and Young People’s Transformation Programme e-learning[9] in addition to face to face. Long term, the aim will be to develop “asthma friendly schools” (including those with complex needs pupils) and writing a county wide asthma school policy.[10]
Improved access via school: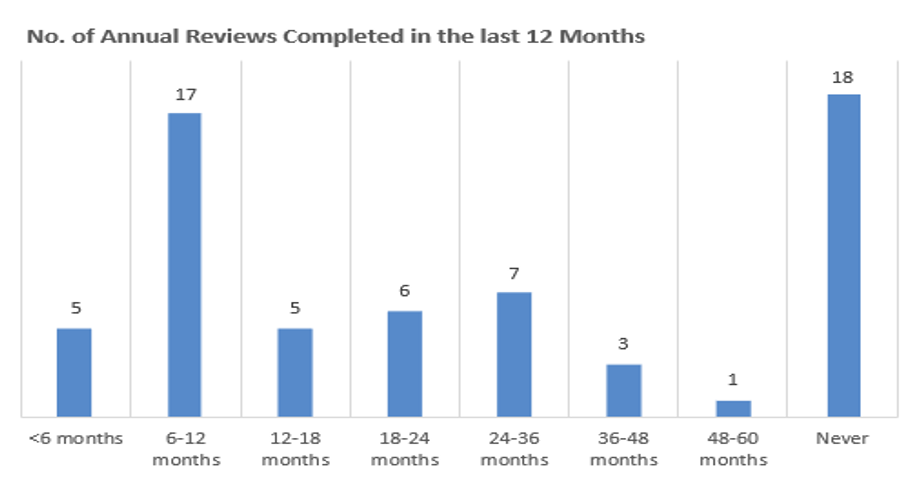
Notably, only a third of the families seen had received a review in the last year (and often this was over the phone). The remaining two-thirds had experienced a significant delay in their review, of either up to five years (35%), or they had never had an asthma review (29%). This means 64% of families that attended school reviews had not had an asthma review at their GP surgery in the past year despite reminders, or they had not been invited to the surgery at all. Of significance, was the large volume (25% of families that attended) with some degree of safeguarding input that chose to access reviews through school.
Holding reviews in schools appears to improve accessibility and therefore significantly increase uptake. This is in deprived areas, where uptake in asthma reviews is especially challenging.[11]
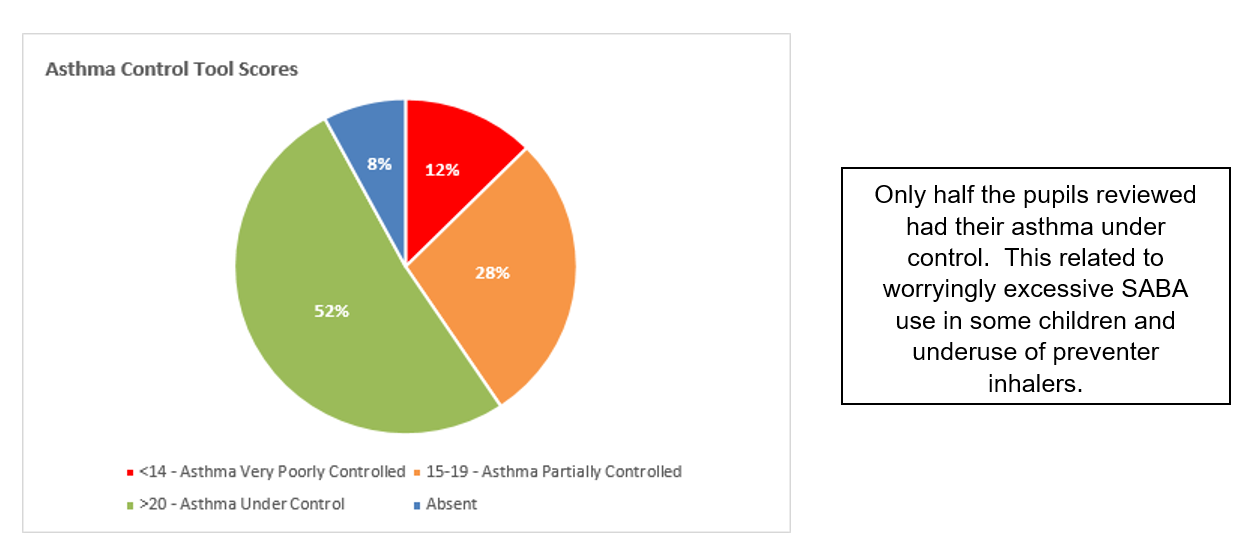
Annual reviews, asthma diagnosis levels and asthma control
The lack of annual review invites coincides with a lack of diagnosis: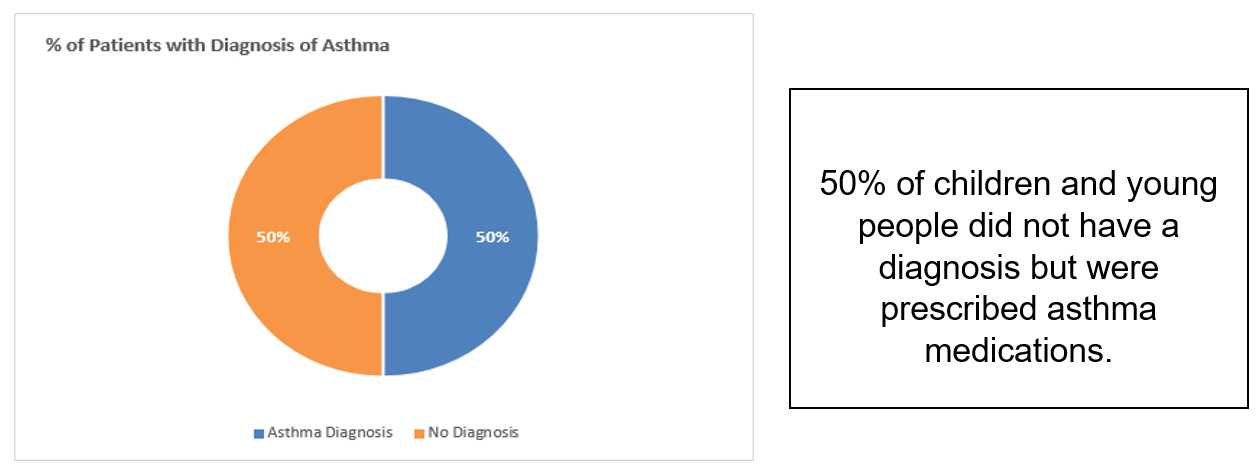
Not having a diagnosis has implications in terms of asthma codes not being generated and therefore impacts on care provided (including invites to annual reviews) and corresponding poor asthma control.
Inhaler Technique, PAAP and Inhalers / Spacers at school
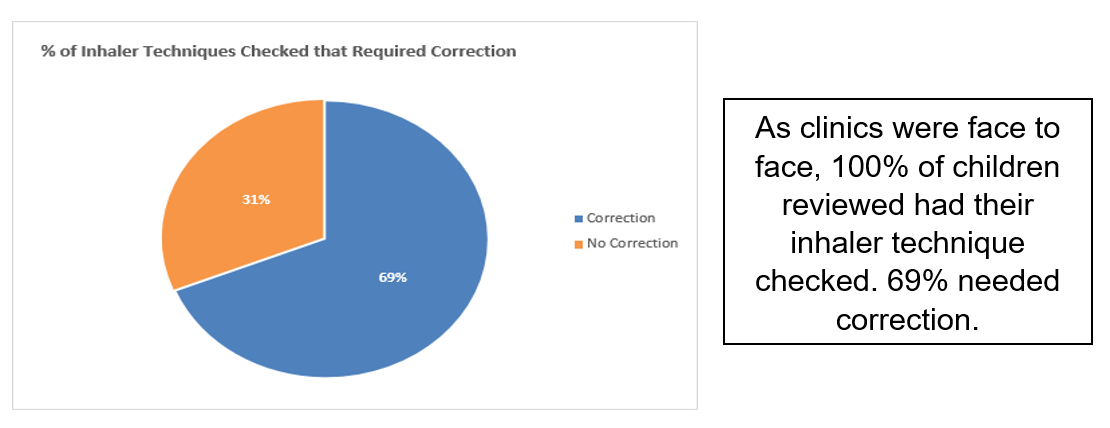
Of concern was the large volume of children with incorrect inhaler technique:
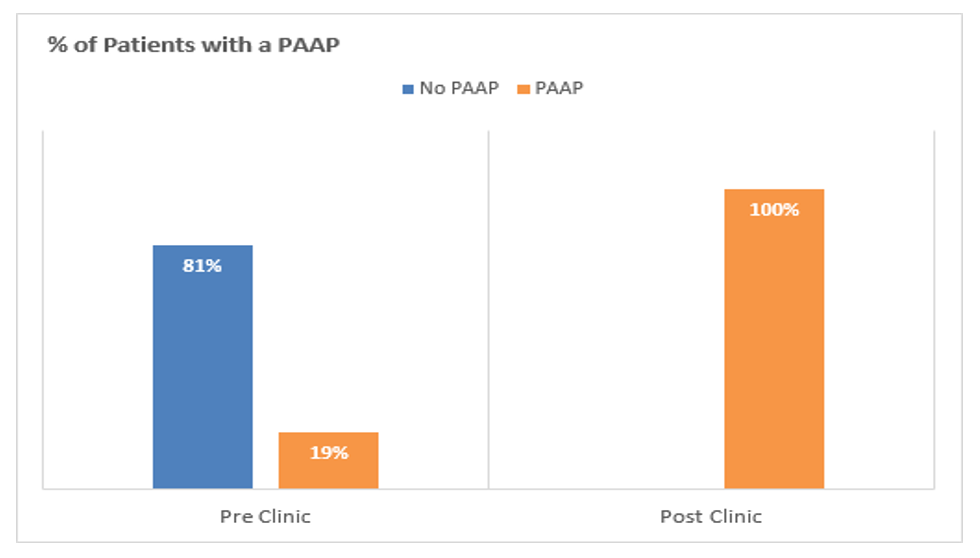
 As we have noted, research suggests annual reviews and a personal asthma action plan (PAAP) half the incidence of hospitalisation. Before the clinics, 81% of children did not have a PAAP. After school clinics, 100% of children received a PAAP. Schools also received a copy. Prior to clinics no schools had a PAAP.
As we have noted, research suggests annual reviews and a personal asthma action plan (PAAP) half the incidence of hospitalisation. Before the clinics, 81% of children did not have a PAAP. After school clinics, 100% of children received a PAAP. Schools also received a copy. Prior to clinics no schools had a PAAP.
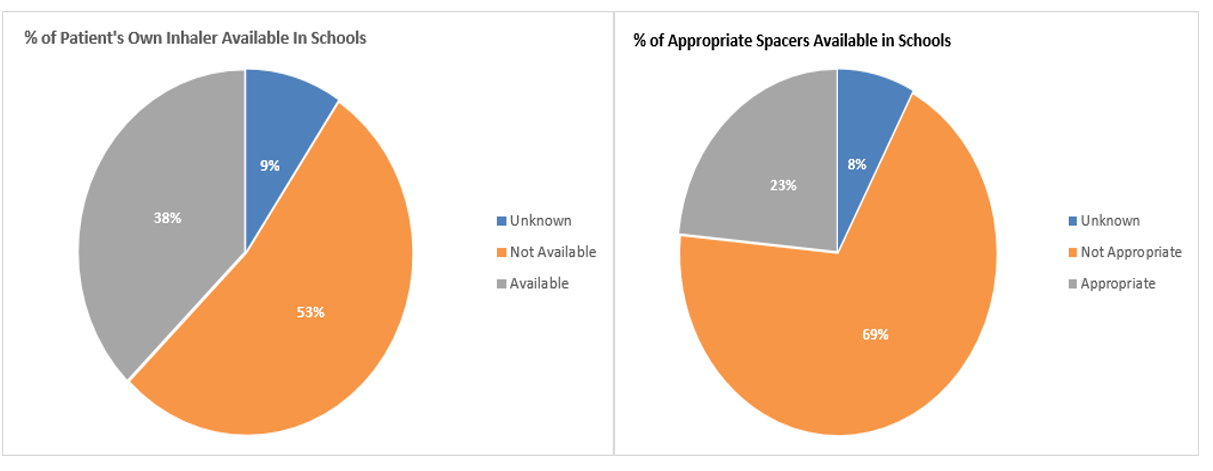
Other issues that became apparent were that only 53% of children had their own reliever inhaler at school, and 69% of children did not have the appropriate spacer at school, (eg not at all, or frequently incorrect size: infant spacer for a 9 year old etc.).
The response post clinics from families was very positive:
- “I think having this appointment is brilliant and gives a fantastic opportunity to talk to somebody about my child’s asthma after not being able to visit the doctors for so long. The lady we saw was amazing and really explained everything clearly and in depth. We all have a much better understanding”
- “This has been great as I had a lot of trouble getting an asthma nurse and getting any help when I really needed it. There was a month wait!”
- “I have had asthma for 8 years myself and learnt loads today which didn’t know. At all the reviews I had not been told why to take the brown inhaler”
- “Myself and my son have both learnt so much today. It’s good to do together and learn together. So helpful and I haven’t had all explained before like this. Very happy”
- “School should be more aware of asthma ….no one could help when my son had an attack”.
- “My child used to refuse to use their spacer, but now they know why, they use it”
School response:
- “We were thrilled with how it went and the feedback from parents has been 100% positive. One parent even commented that it has changed his life already as his breathing is so much better now you have reviewed him and have his asthma properly managed……I would be VERY keen to repeat this next autumn term, so if this continues could we please be involved.”
Future direction
Thanks to funding from the ICB, we are now expanding across Norfolk and Waveney, again using the Health of the Nation 2022 heat maps to guide our focus.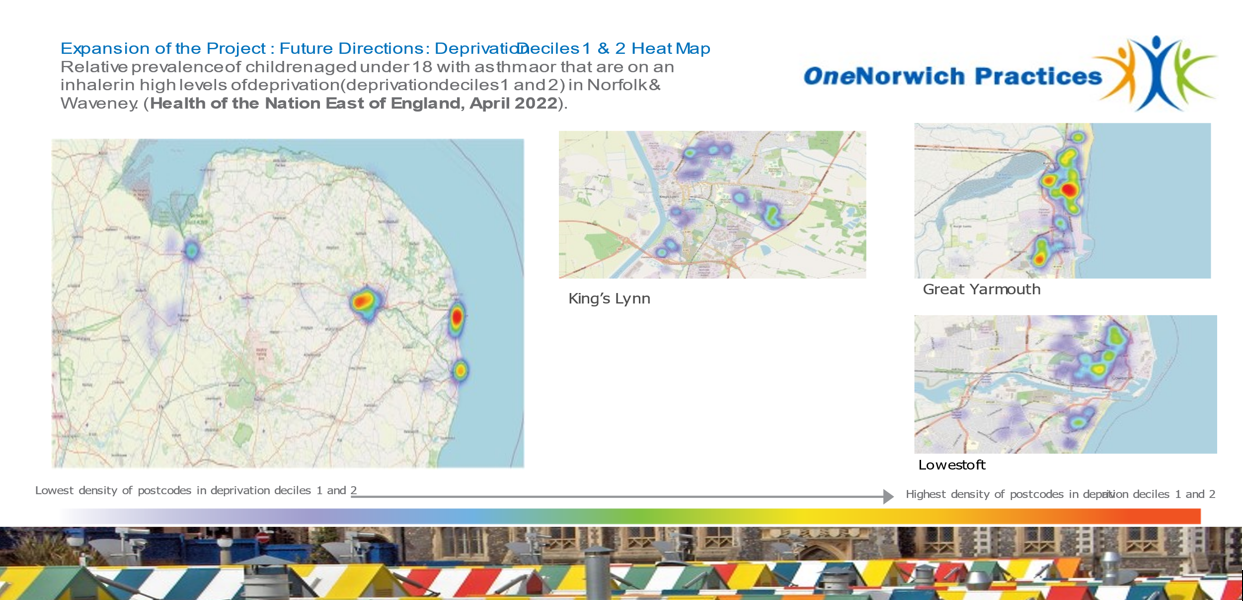
And as we close this blog, we share a final response from one child….
“Can you tell me when you use your inhaler?”
“When my ears are sore”.
By Gina Eyles, Children’s Asthma Nurse Specialist
OneNorwich Practices
References
[1] https://www.asthma.org.uk/support-us/campaigns/publications/inequality/
[2] https://thorax.bmj.com/content/70/Suppl_3/A202.2
[3] (Kossarova et al, 2017) https://www.nuffieldtrust.org.uk/research/admissions-of-inequality-emergency-hospital-use-for-children-and-young-people.
[4] Royal College of Physicians, 2014, Why Asthma Still Kills The National Review of Asthma Deaths, http://www.rcplondon.ac.uk/sites/default/files/why-asthma-still-kills-full-report.pdf
[5] (Pinnock, 2015) https://rdcu.be/cS3iX
[7] Levy, M. 2021 Risks of Poor Asthma Outcome in 14,405 children and young people in London Primary Care Respiratory Medicine 31 (3) https://doi.org/10.1038/s41533-020-00215-7
[8] Health of the Nation, 2022, Health of the Nation Report, 2022 East of England Childhood Asthma Insights to Impact.
[11] https://thorax.bmj.com/content/70/Suppl_3/A202.2
Visit the #AskAboutAsthma 2022 campaign page for more content.