Homeless hostels: A London survey of health and care needs
A survey conducted with homeless hostels across London quantifies level of health and care needs. The participating hostel providers include: St Mungo’s, Thames Reach, the Single Homeless Project, the Salvation Army, Evolve Housing and Support, Providence Row Housing Association, Depaul UK, the Riverside Group and Look Ahead Care Support and Housing.
You can download the open document presentation of the survey and its findings here.
You can also read the full report published in ClinMed journal here.
Jump to section
1. Background and rationale to the survey
Many hostel residents have multiple and complex health and social care needs and are dying young. Previous research highlights:
- Older homelessness is on the rise and had doubled between 2010 and 20151
- High levels of frailty, multiple health problems and conditions associated with older populations within hostels2
- 48% of hostel residents were assessed as having memory problems and other vulnerabilities with a further 19% as borderline3
- Unrecognised palliative care needs with deaths often unsupported, following crisis led admissions4
Hostels are not staffed to provide long term housing or high level of support.
- Clients often do not receive the level of health or social care input they require and few receive an adequate care package
- Can be difficult for hostel staff to advocate for getting care packages
- Hostel staff are not trained in health and are not carers, yet are left to support people with high need.
- Burnout rates amongst staff are high
What is not known is:
- Comprehensive data relating to the social care needs of people experiencing homelessness
- Number of residents regionally who would benefit from alternative places of care
As part of St Mungo’s organisational strategic review they wanted to understand wider needs
St Mungo’s have 2 CQC registered care homes (Hilldrop Road and Chichester Road) but this is not enough for needs across London.5
In order to quantify the level of health and social care needs amongst residents in homeless hostels across London, St Mungo’s developed a health and care needs survey together with Transformation Partners in Health and Care (formerly HLP).
This was rolled out into St Mungos projects (Phase 1) initially and then adapted further and rolled out across the following additional services across London (Phase 2).

housing waiting list and has struggled to find a modified home to suit his needs. He used to
work as a doorman and a manager for a food superstore, and has also supported himself by
selling his paintings. Credit: Jeff Hubbard/PA Wire/Centre for Homelessness Impact.
2. About the survey
Survey aim
To quantify the level of health and social care needs amongst residents in homeless hostels across London within:
- First stage hostels
- Semi-independent accommodation
- Assessment hubs (with accommodation)
Hostels specifically for young people and outreach services were excluded
Methodology
A two phase, cross-sectional survey completed by hostels managers.
- Phase 1 (March 2022): survey co-designed with St Mungo’s and clinician/researcher from Transformation Partners in Health and Care rolled out to St Mungo’s London services, this included 26 services and 1,172 clients
- Phase 2 (September 2022): an updated survey with input from eight additional service providers and rolled out across London, this included 32 services and 1,184 clients
- The surveys contained a combination of quantitative closed questions and opportunity for free text (open questions)
- In total, the survey was completed by a total of 2,355 clients across 58 hostels from 9 different providers
3. Survey findings
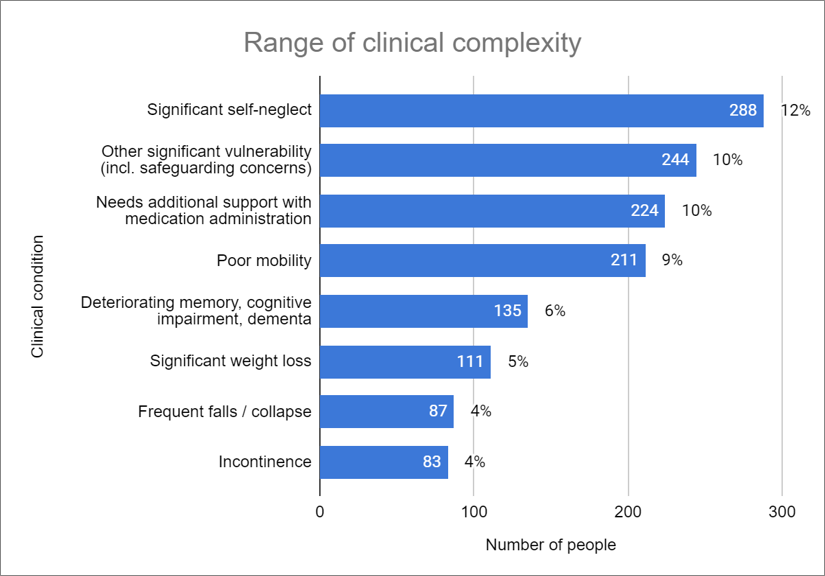
Complexity and vulnerability
- Many long-term conditions similar to found in elderly populations
- 609 (26%) had more than one clinical condition
- 209 (13%) had three or more clinical conditions
- 603 (26%) of clients were deemed to have poor or deteriorating health
Challenges for hostel staff in getting support for their clients
The following themes emerged from free text comments in the survey.
- Opinions not being valued
- Poor discharge planning from hospitals, teams not not involving frontline staff
“Failed discharges due to self discharge or poor discharge planning has led to two residents returning to hospital within 72 hours …. “medically fit” but not able to manage in the community independently.”
Hostel Manager
- Many barriers to access including:
- lack of flexibility from statutory services and non-engagement not recognised as a support need
- Lack of consistency and continuity
- Digital exlusion for example not receiving appointments due not having a phone
- Substance use, a barrier to accessing services, for example mental health support or social care support
“Also mental health services refuse our customer referrals without even assessing them stating it is drug induced when under NICE guidelines they have a statutory duty to accept people with dual diagnosis.”
Hostel Manager
- Eligibility treshold: needs were deemed too high for some services but too low for others
- Environment not designed for supporting those with very high need
Care Act assessments
The following findings were found relating to Care Act assessments.
- 133 Care Act assessments were made by hostel staff in the past year (from 37/58 hostels)
- 72 (54%) responses received were believed to be adequate
- Managers felt 110 (5%) clients needed a personal care package but did not have one, hostel staff felt additional support was needed for:
- Medication management, self care, keeping room clean, supporting nutrition, addressing isolation
- The following challenges emerged:
- Lengthy and complicated process between referral and receipt of support
- Assessments in hospitals often not reflecting realities of life in the community
- Cases closed too quickly if resident was not contactable or refused to see the assessor
- Substance use and self-neglect seen as ‘lifestyle choices’ Eligibility for support for people with restricted or uncertain benefits to public funds
- Eligibility for support for people with restricted or uncertain benefits to public funds
- Hostel staff were often not involved in the assessments and clients may not always recognise their own needs
- The following enablers were found:
- Support from other services and agencies e.g. occupational therapist
- Skilled workforce familiar with the process
“When Social Services contact a resident they state they are fine and don’t require support. Further investigation/room checks …would have been beneficial..”
Hostel Manager
“As we are not equipped with managing clients that require care input, we struggle to get their care coordinators to take the matter to panel. They wait until the damage is done or where they reckon that the situation may present public relations damage, then they act”
Hostel Manager
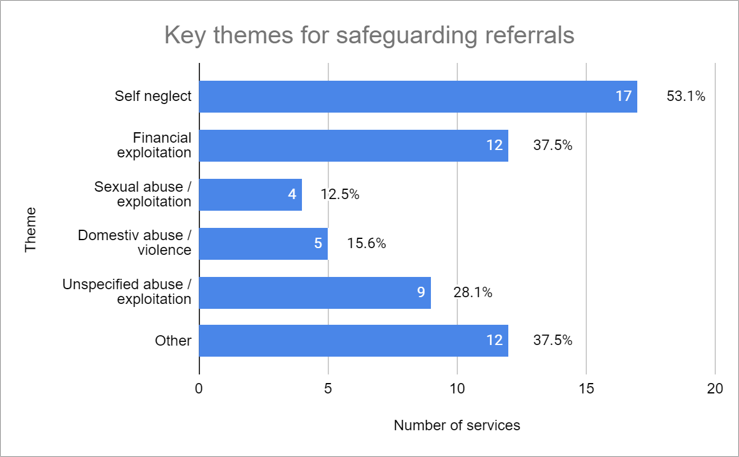
Safeguarding referrals
The following safeguarding referrals in the past year (insert dates) for 257 (11%) clients:
- 55 (41%) clients needed repeated referrals*
- 59 (44%) responses were believed to be adequate*
Hostel staff experienced challenges similar to those noted for Care Act assessments.
*out of 135 referrals (second phase survey only).
Facing the challenges mentioned above could result in a lack of support from adult social care for some of the most vulnerable in society, oftentimes with devastating consequences.
“I have been to 3 serious case reviews when customers died after I have made safeguarding alerts for self neglect, which were rejected by social services citing lifestyle choice. Each review concluded that social services must not reject cases citing lifestyle choice but it keeps happening…
We are left to support the most high risk, complex people with zero support from statutory services. It is disgrace. Homeless people and people who use substances are entitled to services and care but are failed by these services.”
Hostel Manager
Ambulance calls
- 108 (5)% clients had more than three unplanned hospital visits in the previous month
In phase 2, there were further questions regarding call outs in the previous month, including:
- There were 100 callouts for 62 different individuals*
- A small number of residents (4 people) had an ambulance called 3 or more times*
- Some ambulance staff refused to transfer a person to hospital as they deemed the issue was related to substance use rather than mental health; this meant hostel staff were left to support people with significant problems without specialist support*
“We have some clients with mental health related needs that we would consider high – when Crisis team or ambulance is requested to support often they don’t attend, or if they do they leave as it’s felt the client’s behaviour is substance use related rather than mental health.”
Hostel Manager
*Second phase survey only (32 services; 1184 clients).
Move-on options
- 30 (52%) managers said they had no options or rarely had access to move-on options, only one manager reported having adequate move on options
- Waiting lists were long and thresholds for eligibility were high
- Particular problem for those with substance use issues and high care needs
- 25 out of 32 (78%) service managers had one or more individual(s) they believed needed high-support accommodation
- A total of 102 clients (9%) were identified as having needs that were too high for the service they were in*
- Managers felt that there was a need for more:
- Specialist care homes
- Women-only accommodation
- Smaller units for people with mental health issues
- Abstinence based accommodation
- Housing First options with floating support
- Sheltered accommodation
“..there is no pathway into extra care or Sheltered living for people who suffer with long standing substance misuse issues. … with one particular client we have been back and forth for 18 months plus.”
Hostel Manager
“It’s challenging to access the service and homes they need. There is limited information on who to contact, some pathways require bidding however some clients do not have the capacity to do so.”
Hostel Manager
“Need social worker in the pathway, with better route out of hostel for those facing palliative/end of life care. It is sad that those with numerous physical health issues that will likely die in hostels …aren’t given more opportunities to live out their life in sheltered/supported accommodation.”
Hostel Manager
Deaths
- In the last 12 months, managers thought there were 29 deaths (approx 2%)*
- 10 (66%) deaths were believed to to not be related to an overdose, accident or suicide*
- Causes include multi-organ failure, brain haemorrhage, cancer, heart attack, heart failure, infection, liver disease or unknown*
- 10 (66%) deaths were believed to to not be related to an overdose, accident or suicide*
- Location of deaths:
- 15 (52%) in the hostel*
- 8 (28%) in a hospital*
- 2 (7%) in a hospice*
- 4 (14%) in other place not listed or not specified*
- In both phases, there were 225 (10%) clients for whom managers said they would not be surprised if they were to die in the next year from a health condition
*Second phase survey only (32 services; 1184 clients).
4. What managers said was needed
Adult social care
- More support with people who self neglect and use substances and around medication
- Improved communication with social care and safeguarding teams – quicker response and feedback from referrals and assessments, attending MDT’s
- Carers that understood the client group and could deal with difficult behaviours by building rapport with residents
Other services
- To understand the discharge environment, hospital teams should engage hostel staff to ensure appropriateness of discharge location
- Hostel staff’s input in hospital MDT meetings can be valuable to understanding the full scope of individual needs for effective discharge planning
- More consistency, continuity and flexibility in providing appointments and support, such as accepting clients with multiple needs or who failed to attend appointments
- More inreach from nurses/doctors/ occupational therapist / dental services/ mental health and addiction services particularly dual diagnosis
- Reducing barriers to access including digital exclusion
Overall
- A greater range of accommodation options with access to support is needed
- More adult social care and health in-reach/support is needed for many living in homeless hostels
Summary
- This survey has demonstrated significant unmet needs within homeless hostels
- Currently hostel staff are taking responsibility for people with significant health and social care problems without adequate support from statutory agencies
- From the hostels in phase 2, managers believed that overall 9% of their clients had needs that were too high for the service they were in yet there were rarely good move on options
- The percentages of unmet need are not so high that this cannot be addressed
If you would like to know more about the survey, or would like to get in touch with our team, please contact rf-tr.hlp-homelesshealth@nhs.net